



STARR Study Group, Meuffels, D. E., &...
New publication
read more
STARR Study Group, Meuffels, D. E., &...
Arens T, Melick van N, van der Steen MC, Janssen...
Distortion of the knee may lead to instability on the medial side of the knee. This ligament is often referred to as medial collateral ligament (MCL). MCL instability can cause limitations in activities of sports and daily life. An early diagnosis of MCL instability is important because the MCL can heal, if treated adequately. On this webpage, you will read information on the MCL, MCL lesions, treatment and rehabilitation.
Anatomy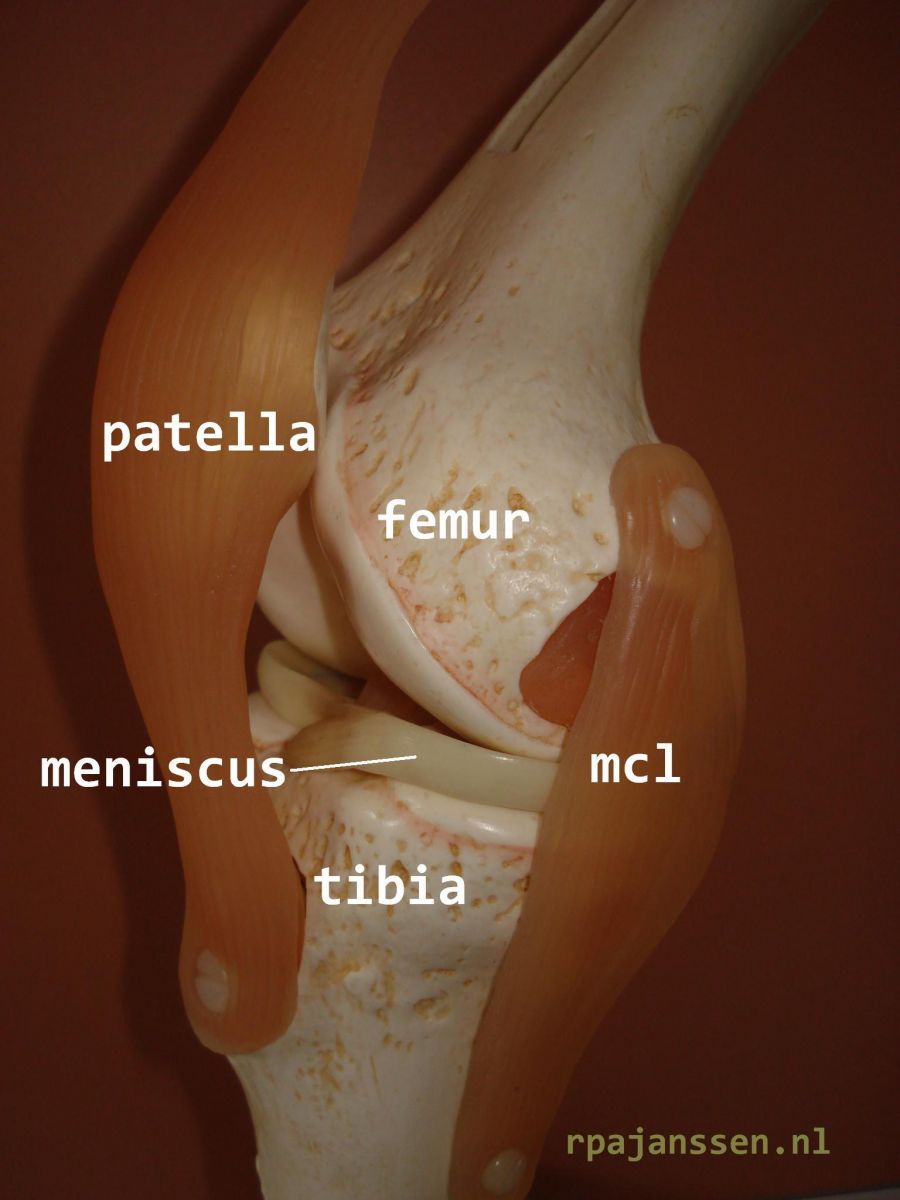
The knee joint is the articulation between the femur and tibia. Bone is covered by cartilage to allow smooth knee motion. The inner (medial) and (outer) lateral meniscus are situated between the femur and tibia as shock absorbers (see Information Meniscus). The medial and lateral collateral ligaments as well as the cruciate ligaments provide stability of the knee joint. The medial structures of the knee (often referred to as MCL) are composed of various components that are responsible for the collateral stability of the medial side of the knee.
Medial knee injuries
A sudden sideways movement of the knee can lead to injury of the MCL. This is often caused by trauma to the knee and sports injuries. Symptoms are pain on the inside of the knee and a feeling of giving way, sometimes accompanied by hematoma. MCL lesions occur in all age groups. They are often accompanied by other knee injuries such as meniscal tears and cruciate ligament injuries.
Treatment
A correct diagnosis is important for treatment, rehabilitation and prognosis for (sports) activities in the future. MCL lesions are categorized in 3 types: MCL grade 1 injury is characterized by merely pain on the medial side of the knee without instability. These lesions heal spontaneously with rest in 4-6 weeks. In case of MCL grade 2 injury, there is moderate instability of the medial side of the knee. MCL Grade 3 lesions show severe instability of the knee. Scientific research has demonstrated that MCL grade 2&3 injuries heal very well if diagnosed early and treated adequately with a knee brace. Treatment is depending on the time interval between the knee injury and diagnosis.
Early diagnosis
If diagnosed within 2 weeks after the knee injury, MCL grade 2&3 lesions are treated with a prescribed knee brace for 6 weeks. This brace can be provided at the Orthopaedic Center Máxima on weekdays, after referral by your general physician (huisarts). The brace needs to be worn 24 hours per day. You can walk and cycle with the brace as it allows full knee range of motion. In the shower, it needs protection by a sealing bag. After 6 weeks, the brace is removed and the knee stability examined at the outpatient orthopaedic clinic. If the MCL has healed adequately, you may return to sports activities.
Late diagnosis
If diagnosed after 2 weeks, MCL grade 2&3 lesions have a tendency to heal less. Brace treatment may be attempted within 4 weeks after the injury. Thereafter, there is a risk of chronic MCL instability.
Wearing a knee brace with sports activities may compensate chronic MCL grade 2 injuries. Chronic MCL grade 3 injuries cause limitations in activities of sports and daily life. In these cases, a surgical reconstruction is recommended to restore medial knee stability.
Anatomical medial reconstruction
Scientific research has shown that chronic MCL grade 3 injuries are best treated with an anatomical MCL medial reconstruction of the knee (technique by Prof. R. LaPrade, M.D. PhD). The two main structures of the medial side of the knee are reconstructed with autograft (if available) or allograft tissue. The new ligaments are fixed in bone tunnels in femur and tibia. RPA Janssen, M.D. is an instructor at annual (inter)national courses to teach the latest surgical techniques of knee ligament reconstructions (see Biography).
After the operation
Hospital stay is 2-3 days. The day after surgery, the physiotherapist will give you knee instructions as well as teach you how to walk with two crutches. You need to limit weight bearing on the operated knee for 6 weeks. During this time, thromboprophylaxis is prescribed. A removable brace is provided for 6 weeks. Knee exercises are important which will be explained to you and can be done at home and at the physiotherapist’ office. You may start with physiotherapy the week after the operation. Patients from the Netherlands are referred to my practice for knee ligament reconstructions. A standardizes protocol can be downloaded for the physiotherapist close to your house (download protocol MCL reconstruction – in Dutch). A referral for your physiotherapist is provided at time of hospital discharge. It is recommended to raise the operated leg a few times a day for periods of 15 minutes to limit swelling of the leg. A hematoma may occur during the first week after the operation, this is normal and will disappear within 2 weeks. The first outpatient clinic appointment is after 2-3 weeks. The skin sutures are absorbable and will disappear automatically after a few weeks.
Work and sports
Rehabilitation time after anatomic medial reconstruction of the knee takes 6-12 months. You may resume an office job between 2 to 4 weeks after surgery. Heavy labor may be undertaken after 8-12 weeks. These are general guidelines: it may take shorter or longer depending on knee swelling and pain. Driving a car is not allowed if you walk on crutches (till first appointment). You may cycle on a home trainer after 4-6 weeks. Jogging is usually possible after 12 weeks if swelling and pain are limited. Return to pivot sports is possible after 6 months. Recent scientific research has demonstrated that return to sports activities is related to the knee cartilage condition as well as other possible knee injuries.
Insurance reimbursement
All orthopaedic treatments at our hospital are reimbursed by Dutch insurance companies.
Complications
Complications after anatomic medial reconstruction are rare: wound disorders, infection, thrombosis, vascular or nerve injuries and arthrofibrosis (scarring of the knee). These complications occur in <1% of patients.
Please contact the hospital: