



STARR Study Group, Meuffels, D. E., &...
New publication
read more
STARR Study Group, Meuffels, D. E., &...
Arens T, Melick van N, van der Steen MC, Janssen...
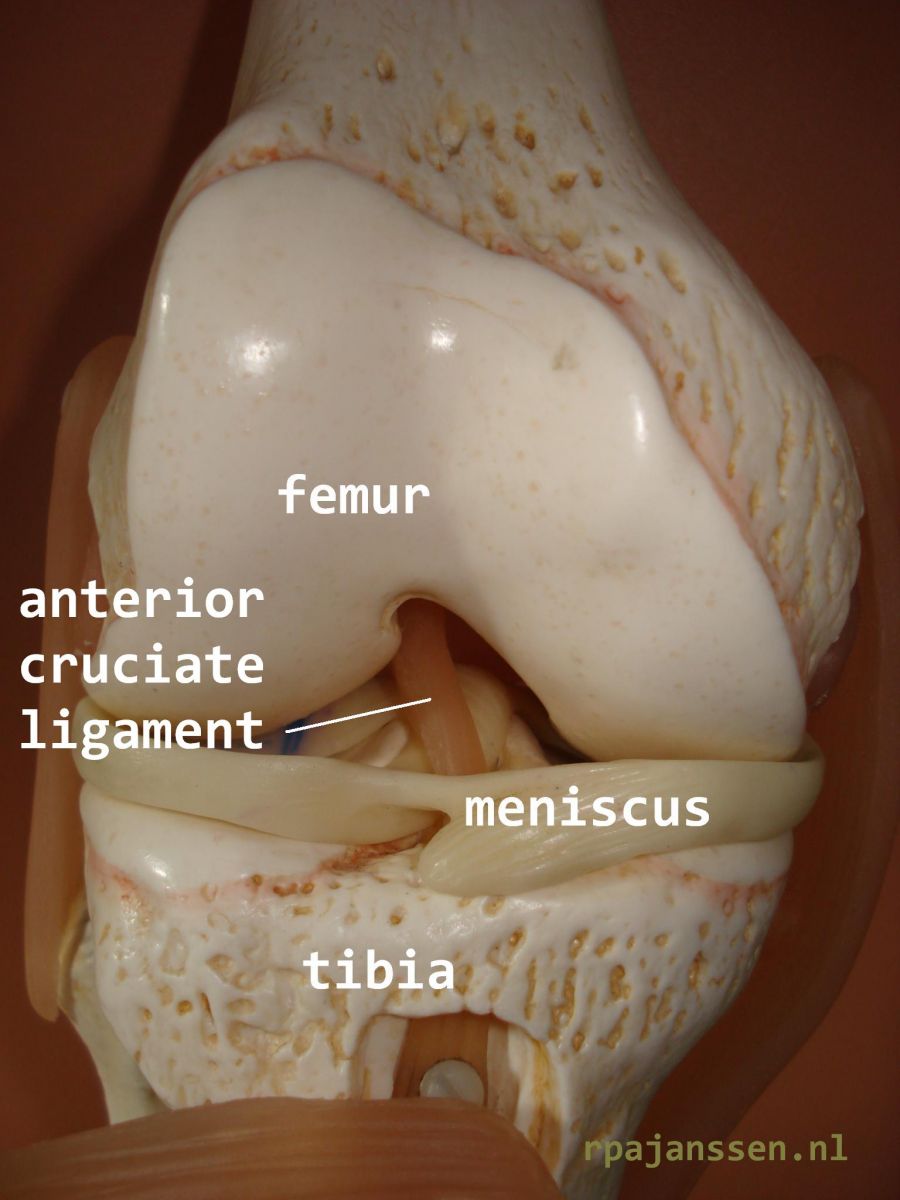
Anatomy
The knee joint is the articulation between the femur and tibia. Bone is covered by cartilage to allow smooth knee motion. The inner (medial) and (outer) lateral meniscus are situated between the femur and tibia as shockabsorbers (see Information Meniscus). Stability of the knee joint is provided by the medial and lateral collateral ligaments as well as the cruciate ligaments. There are 2 cruciate ligaments: the anterior and posterior cruciate ligaments. The anterior cruciate ligament has 2 main functions: restriction of lower leg tibial forward motion as well as excessive rotatory knee movements.
Anterior cruciate ligament rupture
The anterior cruciate ligament ruptures in a forced torsional or hyperextension movement of the knee. The lesion often occurs in pivoting sports such as football (soccer), field hockey or indoor sports. It occurs more frequently in women than men. The acute rupture of the anterior cruciate ligament may occur in patients of wide range in age: the youngest patient in my practice is 5 years old, the oldest 66. The majority of patients is 12-30 years old. In an acute lesion, patients often describe a “popping” sensation in the knee. Anterior cruciate deficient knees often lead to the feeling of giving way in daily or sports activities. Meniscus and other ligament lesions frequently occur in case of cruciate ligament rupture (see information meniscus). It is essential to make a correct diagnosis for adequate treatment, to limit rehabilitation time and optimize the prognosis for future (sports)activities.
Treatment
First of all, other knee injuries need to be adressed and treated. Scientific research has shown that the anterior cruciate ligament consists of 2 separate bundles, each important for specific stabilization of the knee. An anterior cruciate ligament rupture may be total (both bundles are torn) of partial (1 deficient bundle). The necessity for surgical reconstruction of the anterior cruciate ligament is determined by the degree of knee instability as well as (sports)activity requirements of the patient. A nonsurgical treatment by physiotherapy and/or brace may sometimes be sufiicient in patients with limited instability of the knee who do not wish to be involved in pivot sports. Treatment goal is to eliminate the giving way sensation of the knee. 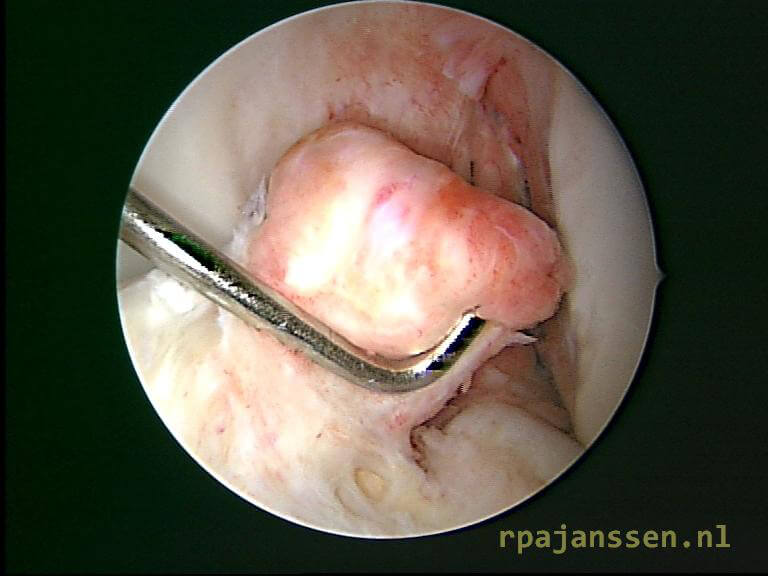
Anterior cruciate ligament reconstruction
A ruptured anterior cruciate ligament does not heal. Reconstruction of the ligament is performed by using hamstring tendon or part of the patella tendon of the same leg. These tendons are very suitable for anterior cruciate ligament reconstruction. My PhD research has demonstrated that hamstring tendons regenerate after their removel for anterior cruciate ligament reconstruction (see Publications). The new cruciate ligament is fixed in femur and tibia through drilled bone tunnels and cortical fixation. This provides a rigid and stable reconstruction allowing accelerated rehabilitation. In case of severe rotatory instabilty or knee laxity, an additional reconstruction (lateral extra-articular tenodesis) is performed on the outside of the knee during the same surgery. Early active exercises are encouraged to allow for better healing. A stabilizing leg brace is not necessary. Recent scientific evidence has shown that a correct surgical technique is essential for good results. In the last 2 years, new anatomic techniques have been developed leading to more than 90% succes rate. I am involved in scientific research on this subject as well as an instructor on a leading, yearly international course for orthopaedic surgeons on knee ligament reconstructions (see Biography).
After the operation
The surgery is usually in daycare. The physiotherapist will give you instructions and teach you to walk with crutches. You are allowed to weight bear as well as bend and extend the knee freely. You will ambulate with the crutches till the first outpatient clinic appointment (2-3 weeks after surgery). Rehabilitation with your own physiotherapist can start within the first week after the operation. A referral will be provided before discharge from the hospital. I operate patients from all over the country. As such, we have developed a proven rehabilitation protocol that can be done by any physiotherapist near your residence (see protocol anterior cruciate ligament: in dutch only). I recommend to lift up your leg during 15 minutes, 5 times daily, in the first two weeks to limit lower leg swelling. For the same reason, you will be given a special stocking to be worn during daytime. The first outpatient check-up will be at 2-4 weeks. The stitches will dissolve by themselves and do not need removal. Experiences of patients are presented in Cases. 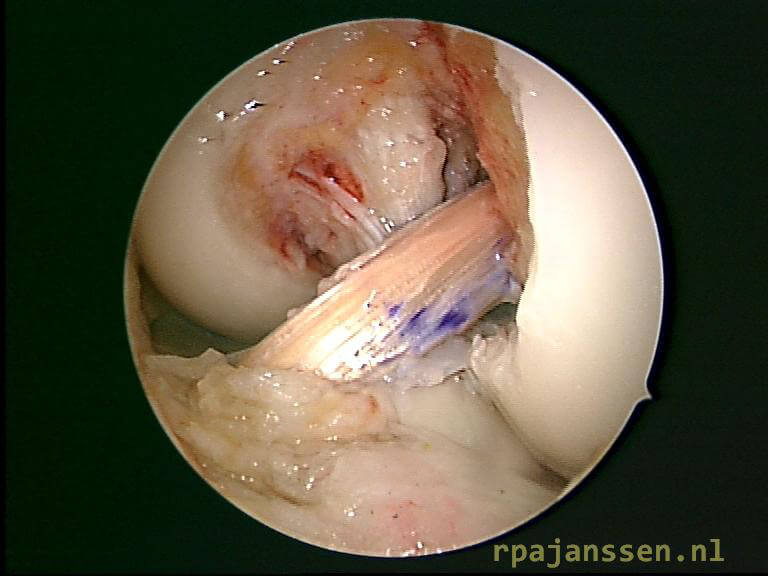
Work and sports
Rehabilitation time after anterior cruciate ligament reconstruction takes 6-12 months. You may resume an office job between 2 to 4 weeks after surgery. Heavy labor may be undertaken after 4-6 weeks. These are general guidelines: it may take shorter or longer depending on knee swelling and pain. Driving a car is not allowed if you walk on crutches (till first appointment). You may cycle on a home trainer if your knee flexes 100º. Jogging is usually possible after 8 weeks if swelling and pain are limited. Return to pivot sports is possible after 6-8 months. Recent scientific research has demonstrated that return to sports activities is related to the knee cartilage condition.
Complications after anterior cruciate ligament reconstruction are rare: wound disorders, infection, thrombosis, vascular or nerve injuries and arthrofibrosis (scarring of the knee). These complications occur in <1% of patients.